
Priyanka Pallapolu
National Research Institute of Unani Medicine for Skin Disorders, ESI x Road, Hyderabad, Telangana, India
Thulasamma Seelamneni
National Research Institute of Unani Medicine for Skin Disorders, ESI x Road, Hyderabad, Telangana, India
Ghazala Javed
Central Council for Research in Unani Medicine (CCRUM), New Delhi, India
Munawwar Husain Kazmi
National Research Institute of Unani Medicine for Skin Disorders, ESI x Road, Hyderabad, Telangana, India
Alokananda Chakraborty
National Research Institute of Unani Medicine for Skin Disorders, ESI x Road, Hyderabad, Telangana, India
Asim Ali Khan
Central Council for Research in Unani Medicine (CCRUM), New Delhi, India
DOI: https://doi.org/10.14456/apst.2025.46
Keywords: Drug Metabolism Temperaments Drug Metabolizing Genes PCR-RFLP Phenotype-Genotype
Abstract
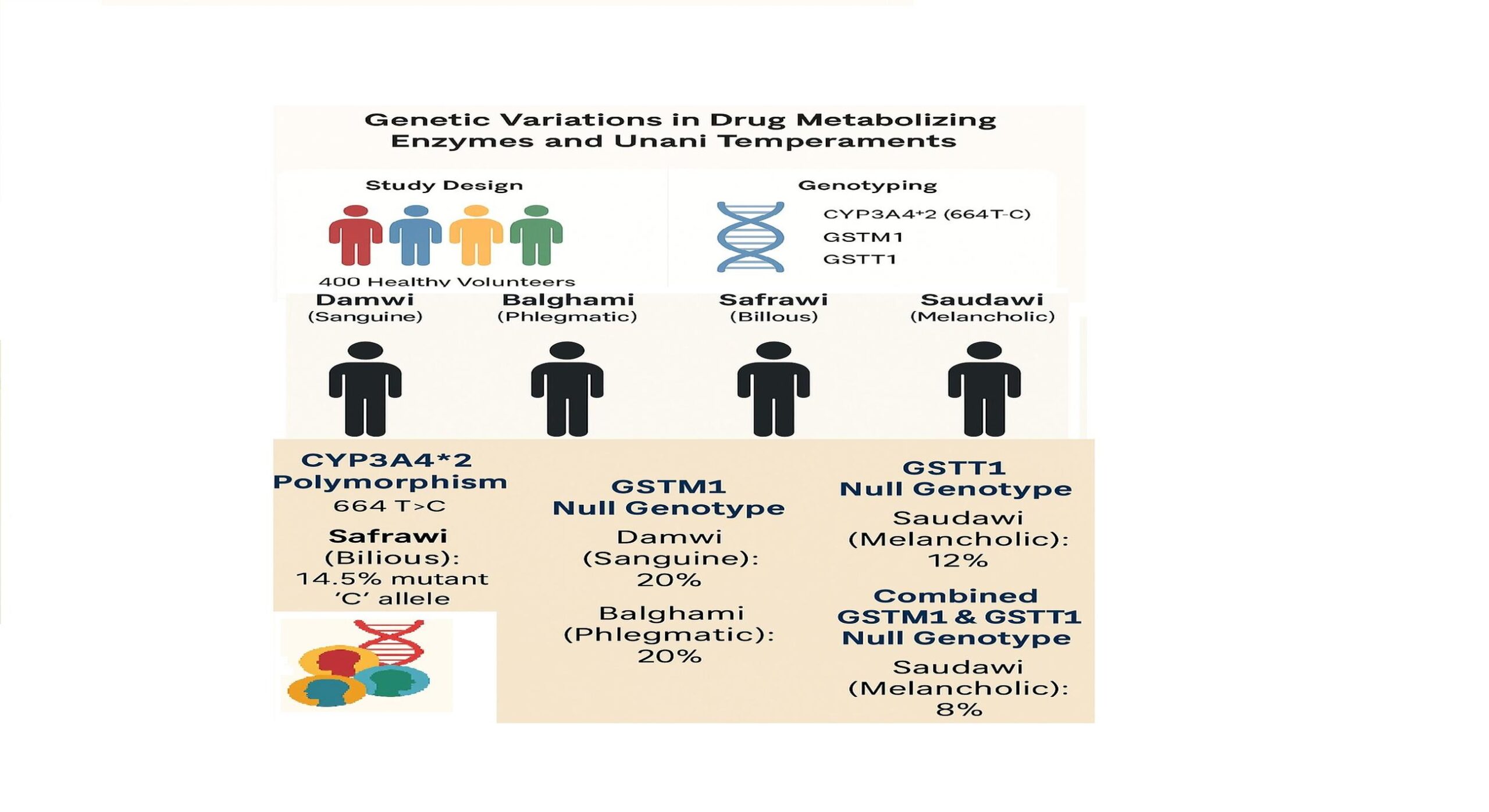
Drug metabolism studies associated with traditional medicine could provide a better insight for understanding the human body differential susceptibility to disease, drug response and even the complex interaction of genetic and environmental factors in disease pathogenesis. Thus, the present investigation is designed to identify the genetic variations in drug metabolizing genes and correlate them with different phenotypes (temperaments) in healthy volunteers according to Unani medicine of philosophy. Four hundred (400 – 100 sanguine (Damwi), 100 Phlegmatic (Balghami), 100 Bilious (Safrawi) and 100 Melancholic (Saudawi)) normal healthy adults of either sex within the age group of 25-55 years formed the subjects of the study. The peripheral blood samples of these individuals were analyzed for CYP3A4*2 (664 T>C), GSTM1 and GSTT1 gene polymorphisms. The frequency of mutant allele ‘C’ in CYP3A4*2 (664 T>C) gene polymorphism was found to be high in Safrawi individuals (14.5%) when compared to other temperament individuals. The GSTM1 null genotypes were high in Balghami (20%) and Damwi (20%) individuals whereas Cytochrome 1 null genotypes were high in Saudawi individuals (12%) when compared to other temperament individuals. In combination analysis both the GSTM1 \ GSTT1 null genotypes were observed high in Saudawi (8%) when compared to other temperament individuals. Based on the assorted polymorphic variations obtained from the study, it is evident that there were differences in the metabolic activity of different phenotypic clusters (temperaments). Thus; the study brings out the possible phenotype-genotype correlation which would be useful in future pharmacogenomics and personalized medicine concepts in traditional medicine.
How to Cite
Pallapolu, P., Seelamneni , T., Javed, G., Kazmi, M. H. ., Chakraborty, A., & Khan, A. A. (2025). Drug Metabolic Variability of CYP3A4*2, GSTT1 and GSTM1 gene polymorphisms and its correlation with clinical phenotyping in South Indians. Asia-Pacific Journal of Science and Technology, 30(03), APST–30. https://doi.org/10.14456/apst.2025.46
References
World Health Organization. Constitution of the World Health Organization. In: World Health Organization: Basic documents. 45th ed. Geneva: WHO; 2005.
Azmi WA. Moalijaat jild doom. Amraz-e nizam -e-hazam we tawleed we tana sul [Treatments volume two: Diseases of digestive, reproductive and urinary systems]. New Delhi: Faroog Urdu Bawan, Wazarate Terqi Insane Wasail Hakumat Hind; 2012. p. 207.
Arzani MA. Tibbi-e-Akbar. Deoband: Faisal Publication; 2002. p. 739.
Jabin F. A guiding tool in Unani Tibb for maintenance and preservation of health: a review study. AJTCAM, 2011;8(5S);140–143.
Duster T. Medicine. Race and reification in science. Science. 2005; 307(5712):1050-1051.
Braun L, Fausto-Sterling A, Fullwiley D, Hammonds EM, Nelson A, Quivers W, Reverby SM, Shields AE. Racial categories in medical practice: how useful are they?. PLoS Medicine. 2007;4(9):e271.
Johnson JA. Ethnic differences in cardiovascular drug response: potential contribution of pharmacogenetics. Circulation. 2008; 118(13):1383-1393.
Omiecinski CJ, Vanden Heuvel JP, Perdew GH, Peters JM. Xenobiotic metabolism, disposition, and regulation by receptors: from biochemical phenomenon to predictors of major toxicities. Toxicol Sci.; 2011; 120 (Suppl 1): S49-S75.
Nebert DW, Russell DW. Clinical importance of the cytochromes P450. Lancet; 2002; 360:1155–62.
Floyd MD, Gervasini G, Masica AL, Mayo G, George AL, Bhat K, Kim RB, Wilkinson GR. Genotype-phenotype associations for common CYP3A4 and CYP3A5 variants in the basal and induced metabolism of midazolam in European- and African- American men and women. Pharmacogenetics; 2003, 13:595–606
Danielson PB. The cytochrome P450 super family: biochemistry, evolution and drug metabolism in humans. Curr Drug Metab; 2002, 3:561–597.
Zanger UM, Schwab M. Cytochrome P450 enzymes in drug metabolism: regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol Ther. 2013, 38: 103–141.
Kadlubar FF, Berkowitz GS, Delongchamp RR et al. The CYP3A4*1B variant is related to the onset of puberty, a known risk factor for the development of breast cancer. Cancer Epidemiol Biomark Prev; 2003;12:327–331.
P. Yadav, A. Chatterjee, and A. Bhattacharjee. Identification of deleterious nsSNPs in 𝛼, 𝜇, 𝜋 and 𝜃 class of GST family and their influence on protein structure. Genomics Data, 2014;2:66– 72.
M. A. Garc´ıa-Gonz´alez, E. Quintero, L. Bujanda et al. Relevance of GSTM1, GSTT1, and GSTP1 gene polymorphisms to gastric cancer susceptibility and phenotype. Mutagenesis. 2012; 27(6):771–777.
Kim SJ, Kim MG, Kim KS, Song JS, Yam SV, Chung JH. Impact of glutathione S-transferase M1 and T1 gene polymorphisms on the smoking-related coronary artery disease. J Korean Med Sci. 2008; 23(3):365-372.
Suman G, Jamil K. Novel CYP3A4 Gene polymorphisms in post chemo breast cancer patients. Int J Cancer Res. 2006;2:358–366
Arand M, Muhlbauer R, Hengstler J, Jager E, Fuchs J, Winkler L, et al. A multiplex polymerase chain reaction protocol for the simultaneous analysis of the glutathione S-transferase GSTM1 and GSTT1 polymorphisms. Anal Biochem. 1996; 236:184–6.
Rebbeck TR, Walker AH, Phelan CM, et al. Defining etiologic heterogeneity in breast cancer using genetic biomarkers. Prog Clin Biol Res; 1997; 396:53-61.
Kim J, Pham D. Sasang constitutional medicine as a holistic tailored medicine. vid. Based Complement. Alternat Med. 2009;6:11–19.
Chenna, K., E.C. McCanlies and A. Weston. CYP3A4 Polymorphisms-potential risk factors for breast and prostate cancer: A huge review. Am J Epidemiol. 2004;9:825-841.
Kumar, K. and K. Jamil. Methylene tetrahydofolate reductase (MTHFR) C677T and A1298C polymorphisms and breast cancer in South Indian population. Int J Cancer Res. 2006;2:143-151.
Thummel, K.E. and G.R. Wilkinson. In vitro and in vivo drug interactions involving human CYP3A. Annu Rev Pharmacol Toxicol. 1998;38:389-430.
Lynch T, Price A. The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. Am Fam Physician. 2007;76:391–396.
Xue H, Su J, Sun K, Xie W, Wang H. Glutathione S-transferase M1 and T1 gene polymorphism and COPD risk in smokers: an updated analysis. Mol Biol Rep. 2012;39(4):5033-5042.
Published:
License
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.